

When appointments become warnings
How appointments power can become a shadow direction power

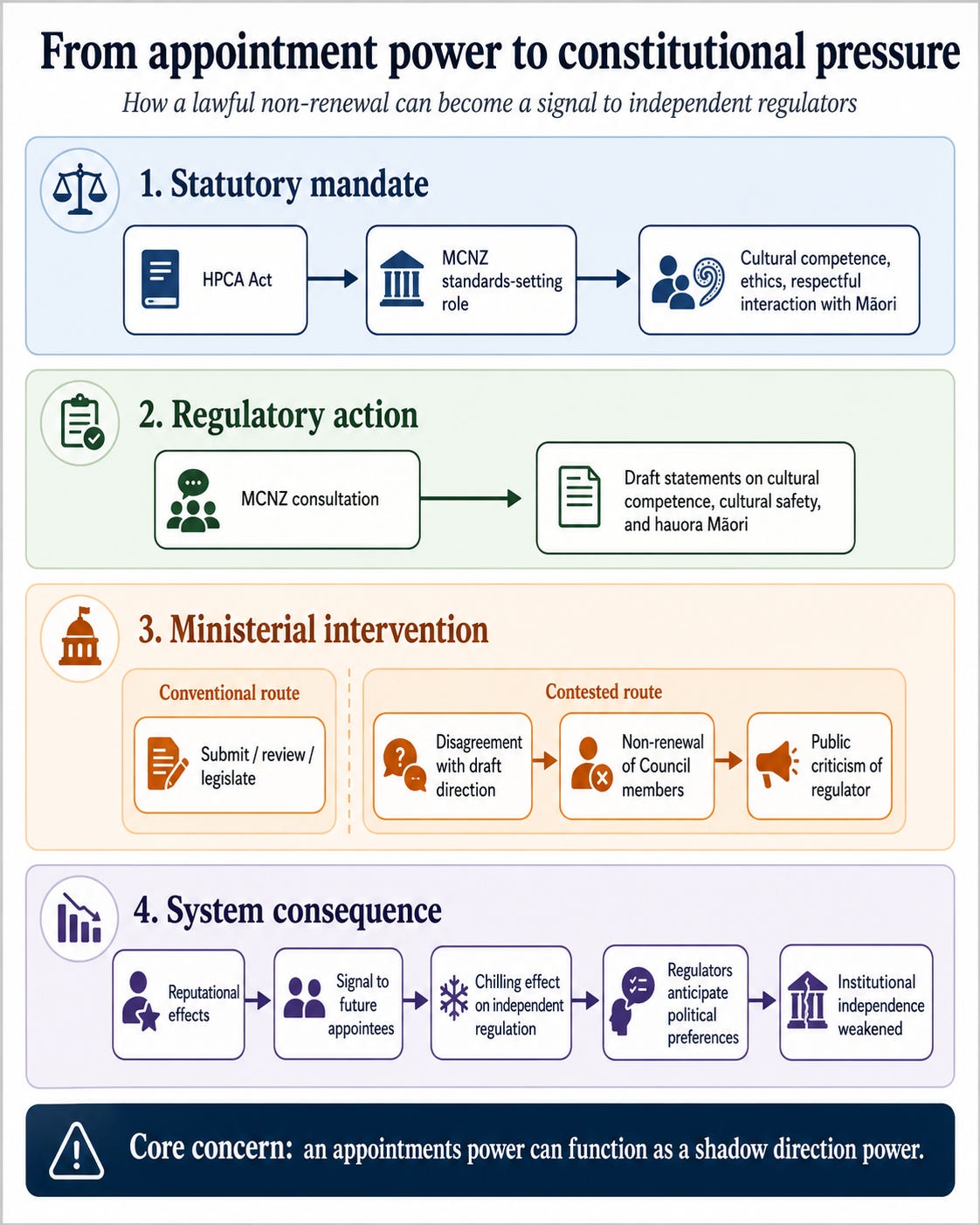
There is a kind of constitutional change that arrives without a headline saying “constitutional change”. No statute is repealed. No court announces a new doctrine. No official says an independent regulator has been captured. Instead, an appointment is not renewed, a public explanation is given, and the rest of the system understands the message.
That is why the dispute over the Medical Council of New Zealand matters. It is not only about Dr Rachelle Love1. It is not only about cultural safety. It is not only about one Minister, one Council or one draft statement. It is about the quiet constitution of healthcare: the settlement by which Ministers are politically accountable, professional regulators remain arm’s-length, and patients are protected by standards that do not swing with the ideological weather.
On the public record, the first discipline is precision. Te Ao Māori News reported that Health Minister Simeon Brown declined to reappoint Dr Rachelle Love and Simon Watt2 when their terms expired, despite both remaining eligible, and said the Medical Council had become distracted by politics and an ideological agenda. The Medical Council later announced Dr Kenneth Clark as chair and Ms Ming-Chun Wu as deputy chair, while acknowledging Dr Love’s leadership and Simon Watt’s service3. The 2022 Gazette notice confirms the earlier three-year terms.
That means the technically safe formulation is not that the Minister formally “removed” the chair. Under the Health Practitioners Competence Assurance Act 2003, Council members are appointed by the Minister, members may be reappointed but not indefinitely, and removal for misconduct or inadequate performance is a distinct statutory mechanism. The Council elects its chair and deputy from among its members. So the decision can be a non-renewal in law while still ending leadership in fact.
This distinction should not make the controversy disappear. It should sharpen it. Appointment power is not a standards power.
The Council’s statutory purpose is public protection through ensuring practitioners are competent and fit to practise. Its functions include setting standards of clinical competence, cultural competence, including competencies for effective and respectful interaction with Māori, and ethical conduct. That phrase is not activist gloss. It is statutory text4.
The Council’s 2026 consultation on cultural competence, cultural safety and hauora Māori may deserve criticism5. Standards should be clear. They should not require doctors to confess political sins or recite fashionable language. They should regulate professional conduct, communication, judgement and safety. They should not become a loyalty test.
That is the strongest version of the Minister’s defence, and it deserves to be taken seriously. ACT welcomed the decision as a reset and urged the Council to withdraw the draft cultural safety guidance6. Democracy Action similarly argued that respectful care is legitimate but that draft wording about privilege, colonialism and systems risks ideological compulsion7. Those objections cannot be dismissed merely because they are politically inconvenient. A regulator that writes unclear standards can chill doctors just as surely as a Minister can chill regulators. That is why they consult.
But the other side of the ledger is stronger. The subject matter itself is not outside medicine. The HDC Code of Rights gives consumers rights to respectful services that take account of cultural, social and ethnic needs, including Māori needs 8; to services of an appropriate standard; and to effective communication. The Pae Ora Act still speaks of equity, culturally safe and responsive services, and a representative workforce. The Government’s own Policy Statement on Health 2024-2027 includes a skilled and culturally capable workforce9.
The literature is also more serious than the slogan “ideology” suggests. Curtis and colleagues’ 2019 review argued that cultural safety is required for health equity and must be linked to power, bias, organisational accountability and patient-defined safety. Their 2025 refinement records how regulators and training bodies are increasingly incorporating cultural competence and cultural safety. Tipene-Leach and colleagues’ 2024 NZMJ viewpoint traces cultural safety from nursing and medical education into Medical Council standards and specialist training.
Mannes, Thornley and Wilkinson’s work on international medical graduates shows why culture is not abstract: it affects adaptation, vulnerability, complaints, support and retention. And, as I will show in coming weeks, this is not solely a New Zealand perspective nor New Zealand evidence. The focus of Medical Regulation in all high-income countries is public safety. Cultural safety is cited equally in each of them. As a Medical Administrator I see the real consequences, including avoidable harm and death, from a lack of cultural safety. Not as a rare event, but regularly.
The policy problem is therefore not “culture versus patients”. Culture is “what we do around here”. Culture is one of the ways patients experience safety, trust, explanation, consent and follow-up. The problem is how to write standards that are rigorous enough to matter and restrained enough not to become coercive.
That is why the method of intervention chosen by the Minister matters. If the draft guidance was poor, the Minister could have submitted to consultation. If the Council was underperforming, the Act contains review, information and audit mechanisms. If the Government wants to narrow cultural competence obligations, it can amend the Act. If it wants greater power over regulators, it can make that case openly through the HPCA Amendment Bill. Ministry materials on that reform already show the central tension: streamlining and patient focus on one side, regulator independence and appointment-power concerns on the other, as summarised in Putting patients first. In a narrower, specific and different (medicines) regulatory sense, I have also made the argument for balancing upstream with downstream regulation.
Public appointments are not meant to be opaque political lightning strikes. CabGuide sets out appointment and reappointment processes, and Public Service Commission guidance contemplates briefings on expiring terms, eligibility for reappointment, skills and succession planning. Those materials may ultimately vindicate an ordinary governance explanation. But until the appointment papers, recommendations and reasons are released, the public is left with the Minister’s rhetoric and the timing.
The reputational question should be framed carefully. The public record supports institutional disparagement with foreseeable personal spillover more clearly than it proves a personal shaming campaign. Still, when named leaders are not reappointed and the regulator is publicly described as politically distracted, a reputational cloud falls somewhere. Ministers have every right to criticise regulators. They also have a duty to be accurate, evidenced and proportionate, because their office gives their words institutional force. On the evidence, the minister was not only inaccurate, he has sanctioned the Medical Council of New Zealand for executing their core statutory function- not by intent, not interpretively, but by statute:
118 Functions of authorities
(1) The functions of each authority appointed in respect of a health profession are as follows:
…
(i) to set standards of clinical competence, cultural competence (including competencies that will enable effective and respectful interaction with Māori), and ethical conduct to be observed by health practitioners of the profession
That is unambiguous. Parliament decided to include cultural competence in 2003. Minister Seymour Brown in 2026 decided to sanction the Medical Council for executing its statutory function. If I put a red-face emoji here, I’m not sure people will get it. But there should be a red-face emoji here, labelled “Yes, Minister”.
The deeper economic issue is trust. Independent regulation is a commitment device. It tells patients, doctors, overseas regulators, insurers and the public that competence standards are not simply electoral artefacts. If regulators learn that politically exposed standards may cost leaders their positions, they will adapt. This effect is called “crowding out”. They will avoid difficult subjects. Good people may decline appointment. Māori patients and Māori doctors may hear that cultural safety is optional until politics changes10.
The final judgment should be calibrated. The Minister may have acted within the narrow law of non-reappointment. There is no automatic entitlement to another term. Regulators should not become self-perpetuating guilds. Draft standards must be scrutinised, including for clarity, conscience and proportionality.
But a lawful appointment power can still be used in a constitutionally damaging way. Just because something is within the rules, doesn’t mean it was a good idea. The danger is not only what happened to two people. It is the signal sent to every regulator: do not set standards the executive dislikes. That is not consumer or public-centred government. It is standards by appointment threat.
That is to say, the Minister sanctioned Medical Council of New Zealand for undertaking their statutory duty, whilst under consultation about the matters for which he has taken issue with, whilst his Ministry is preparing to submit legislation related to this, and therefore contradicting an existing decision by Cabinet, that unless or until this legislation is passed, this is a matter for parliament to decide.
The better settlement is demanding and democratic: publish the reasons, release the appointment advice, debate the draft standards on their merits, protect doctors from ideological compulsion, protect patients from culturally unsafe care, and preserve the independence of the body Parliament entrusted with competence standards.
Cultural competence should not become an oath of political loyalty. Ministerial appointment power should not become a quiet weapon against statutory standards.
I don’t know Dr Love. We have briefly interacted with relation to a cluster serious adverse event. Ironically, a very serious incident that Minister Simeon Brown has refused to claim any accountability for. I am using Dr Love’s name here, not to pile on. In fact, the opposite. This footnote is written that for the avoidance of doubt, my assessment is that Dr Love was not only doing what MCNZ and the Minister had asked her to do, but she was acting directly within her statutory remit. There should be no loss of dignity for her Mahi.
Mr Watt is a barrister, was a lay member and deputy of MCNZ. Though not commonly talked about, the lay/consumer role on health practitioner regulators is often the hardest. There is a technical mountain to climb. There is a cultural mountain to climb. Medical regulation is not like other health professions. It is not like law. There are very common and real questions about whether the actions of a medical professional put the public at risk. For instance, if the practitioner thought they had seen lividity, cool limbs and felt no pulse, was their decision to not offer CPR, consistent with accepted professional standards. The question of whether it was negligent, is almost entirely a legal question. The question of whether it put public safety at risk is almost entirely a medical question. There are hard question that very few medical practitioners, let alone members of the public, ever have to face. This role will have been a journey for Mr Watt.
Dr Clark is a Obstetrician and Gynaecologist, as well as a Medical Administrator. His background is well suited to this role. Few would be aware quite how dark a place Obstetrics can be. Obstetricians do more acute “life and death” surgery than any other speciality, with the highest expectations and some of the most challenging evidence base.
I opted to exclude from the main text, the point that whilst in New Zealand we have an important reason to prioritise Māori in discussions of cultural safety, the concept is universal. There is a commonly accepted frame, that modern New Zealand has Western European, specifically English origins. I’m not here to point out the Māori side of that story- I’m neither an expert in it, but it’s also not related to my point. That Anglo-centric story is incorrect. New Zealand was administratively managed under the governance of New South Wales. A penal colony dominated by convicts from the states now known as the UK and Ireland. Kiwis, like South Australian’s, like to revise that story, frame ourselves as being formed by free men. Not penal labout. Many conveniently forget the role of Chinese settlers, that Irish culture was and remains vastly different from English culture, in many ways.
In what ways? The uncomfortable truth for Kiwis is the areas we are different are the areas we do not discuss- for example, our expectations of death and dying. Within the UK. Between the UK and Ireland. Between Western and Eastern Europe. Across the planet. I currently help a community with Macedonians who are white. They are Caucasian. Their expectations of death and dying are vastly different. When I talk with Kiwi parents of a dying child, or British, or Scottish, or French, or German, I talk to them differently. Not because I’m woke, but because I’m about to tell them one of the hardest thing in their lives. I want that to be less bad for them. And if I’m honest, I don’t want to end up in front of the medical council for the next five years, because of how I handled a difficult conversation.
Cultural safety and cultural competence isn’t woke. It’s not exceptionalism. It is not racist. It’s espoused in every high income health practitioner regulatory system, because it is disappointingly pragmatic. I find myself finishing this unexpectedly long soliloquy realising that even my attempt to cover a relatable perspective for people who seem like a “bull to a red rag” around anything attempting to improve Māori outcomes, that I’ve not covered other groups, like religion, spirituality, sexual orientation, geez, even educational background…
I don’t have a view.
Let’s be clear. The Deputy Prime Minister and ACT Leader, requested that the peak public safety professional regulator in New Zealand (in terms of raw mortality impact), made a public request going around the Minister of Health, for the Medical Council to cease engaging in a core legislated statutory function. Pause on that. Whatever your political views, ask yourself whether you think that is proper.
As I note below, the consultation is technically ongoing, so it would also technically be inappropriate for the medical council to have responded to their submission at this stage.
This might call out Māori for attention, but by the numbers, raising concerns about these standards is exercised far more by non-Māori, than by Māori. An inconvenient truth not told by any one of these groups claiming Māori get special treatment.
To revisionists, that document was signed by the Minister in the current coalition government.
This effect and problem is even worse in New Zealand, because health practitioners can be sanctioned by MCNZ, by HDC, by HPDT and in the worst cases, by police. But because New Zealand has no personal injury torts, and because in 1961 New Zealand effectively removed serious maladministration and misfeasance (the only high income country to do so), non-clinical managers, executives, boards and ministers, have virtually no mechanism for recourse. This is the ultimate definition for moral hazard (an economic, not a “woke” term).

Interesting perspective thanks.